
Private equity in: Ambulances

This is the first newsletter of my several-part series on private equity in various areas of health care. If there’s an area you think I should cover, reply to this email or hit the comment button.
Private equity has entered into a lot of discrete spaces in medical care:
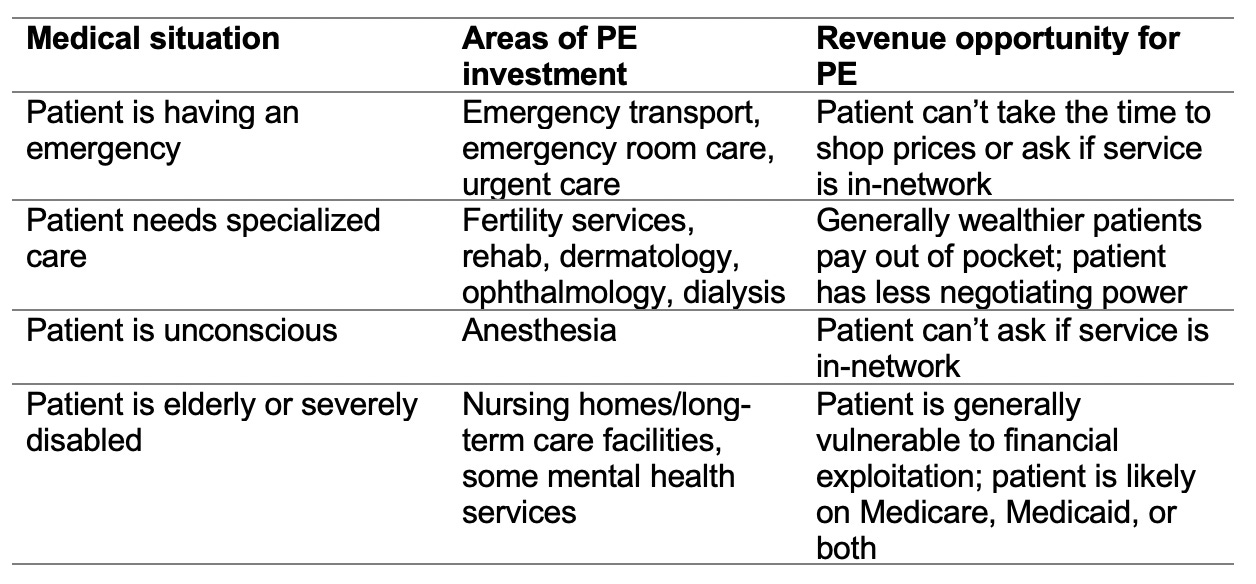
Emergency medical transportation is the first topic I’ll be covering. And next week: private equity in women’s health and fertility services.
In a piece I wrote for the American Prospect last year, I opened with a story that I still think about every time I see an ambulance:
On July 2, 2018, a Boston woman fell into the gap between a subway car and the platform. Passengers rocked the train back and forth, eventually extricating her. Her leg was cut down to the bone. Still, she begged her rescuers not to call an ambulance. “Do you know how much an ambulance costs?” she sobbed. Because there was no choice but to call an ambulance, though, one eventually arrived.*
Emergency transport is one of the most opaque areas of health care. Patients have no control over which ambulance comes in response to their 911 call. And that creates an opportunity for private equity price-gouging.
Private equity’s move into ambulances
In 2008, as the financial crisis took hold and localities began struggling to fund basic services, private equity began aggressively moving into the ground and air ambulance space. Many localities that once ran their own, nonprofit ambulance teams are now serviced by one of a few massive corporations.
Today, just three air ambulance companies control two-thirds of the U.S. market. Two of these—AMR, owned by KKR, and Priority Ambulance, a portfolio company of Enhanced Equity Funds—are private equity-owned.
Rising prices
As private equity’s market share increased, prices also went up. According to a 2019 GAO report, between 2012 and 2017, the median charge for an air ambulance transport increased by over 60%.
The exposure of patients to huge bills also increased. The majority of ambulance corporations strategically refuse to contract with insurers. As a result, more than two-thirds of patients in air ambulances are out-of-network.
This strategy allows air ambulance companies to bill insurers exorbitantly for out-of-network charges and then also bill patients for the remainder. Patients able to pay thousands of dollars up front might do so immediately. Patients unable to pay may take out loans or ask their insurer to make additional payments. But once a patient has exhausted their options, the air ambulance company might well give up on trying to collect. According to reporting in Vertical, an industry magazine, the CEO of Air Methods noted in an earnings call that the company collects “very little” from individuals. Instead, “when we get to the point where we know that we are just working with the patient [instead of the insurer], we will work very quickly to get the account wrapped up.”
While exact figures aren’t available, this strategy of staying out-of-network and scaring patients almost certainly nets air ambulance companies more revenue than if they contracted with insurers.
The amount of patient exposure is striking. A study by University of Michigan researchers found that almost 75% of patients in air ambulances are at risk for a surprise bill, with a median bill amount of almost $22,000. Patients who take ground ambulances are relatively lucky; while nearly 80% of them are at risk for a surprise bill, the median surprise bill is around $450.
Lower quality
A combination of relatively low patient payments (at least compared to the amount billed) with the focus of many private equity owners on paying dividends to shareholders rather than investing in the business has led to a lower quality of service.
This is partly because PE owners aren’t motivated to invest in their business. As I wrote in the American Prospect, the ground ambulance company Rural Metro Fire shows how transfer between PE firms, and the skewed priorities of private equity owners, can be devastating for patients.
The company, also known as Rural/Metro Corporation, was bought by Warburg Pincus in 2011. Rural/Metro then filed for bankruptcy two years later. Oaktree Capital Management, a stakeholder, invested additional money, eliminating Warburg Pincus’s stake. Rural/Metro was then bought by Envision and Global Medical Response, both of which are portfolio companies of KKR. During this time, according to the New York Times, there were formal complaints about a lack of ambulances, county-imposed penalties for late responses, and at least one canceled contract due to a late response that may have contributed to a death.
The low quality of service—and increasingly higher prices—is also partly caused by a distortion in the market. At the height of the PE-ambulance investment frenzy, PE owners opened air ambulance bases all over the country. But as the CEO of Air Methods (a PE-owned corporation) confessed in a 2015 investor call, there are now too many helicopters available. Because the fixed costs of air transport are high—helicopter maintenance, standby crews, fresh medical supplies—air ambulance companies have raised their prices as they face more competition for a limited number of calls.
The competition for patient calls is steep, of course, because air ambulance corporations built bases in areas where patients could pay more, not necessarily in the areas of greatest need.


These two maps, from 2003 (top) and 2014 (bottom) show the distribution of air medical helicopters; the bases are primarily located in places with better patient payer mixes, not necessarily the areas of greatest need. Source: https://www.verticalmag.com/features/isskyhighthelimit/
Potential solutions
Solving the problem of ground ambulance price gouging could be as simple as funding state and local budgets. Ambulance services are much like firefighting services; they’re a community necessity that could be staffed by volunteers. If localities were able to fund community services—and block PE-owned corporations from coming in—ground ambulance fees could be dramatically lower.
It is more difficult to legislate local solutions to air medical transport thanks to a holdover of 1970s-era airline deregulation legislation. The Airline Deregulation Act of 1978 prohibits states from regulating air transport—and courts have interpreted the ADA widely to encompass air ambulances.
Some states, like Wyoming and North Dakota (both places with exorbitant air ambulance costs due to their rurality), have experimented with creative options to hem in air medical prices. Wyoming, for example, tried to expand Medicaid coverage for air ambulance services to all state residents, although the Centers for Medicare and Medicaid Services blocked it. But untill there’s a national prohibition on surprise billing (a policy option that Rep. Richard Neal recently blocked), it’s unlikely that air ambulance prices can be capped.
Another answer would be regulating the intrusion of private equity into health care. A few states are experimenting with this (although not yet in ways that would stop ambulance price-gouging). Washington State, for example, has a law requiring hospitals and providers to notify the state attorney general of any merger or acquisition behavior, giving the state AG room to intervene. Washington’s law, however, doesn’t provide for ambulance mergers.
Recently, California legislators proposed a notification law similar to Washington’s that would have given the state AG the power to block acquisitions of health care entities by PE, hedge funds, or larger health systems. It was defeated this month, but similar laws would go a long way towards protecting smaller health care entities and ambulance companies from financier land-grabs.
Until legislators take action against PE involvement in health care and the surprise bills that result, people like the Boston woman in the introduction story will be forced to choose between high prices and rapid care.
*When I originally published this story, the Boston EMS team reached out to dispute the apparent claim that their services are too expensive. To be clear: this story is not attacking the Boston EMS, a nonprofit service that charges reasonable amounts compared to PE-owned services. It’s a story of a woman, severely injured, whose first thought was of the expense of her ambulance.
Nice post Olivia. PE is also impacting dentistry. The industry is consolidating fast.