
The dream of fixing maternity care
and the startups trying to do it

If you’ve spent any time in healthcare, you’re familiar with the devastating statistics of just how bad maternity care in the U.S. can be.
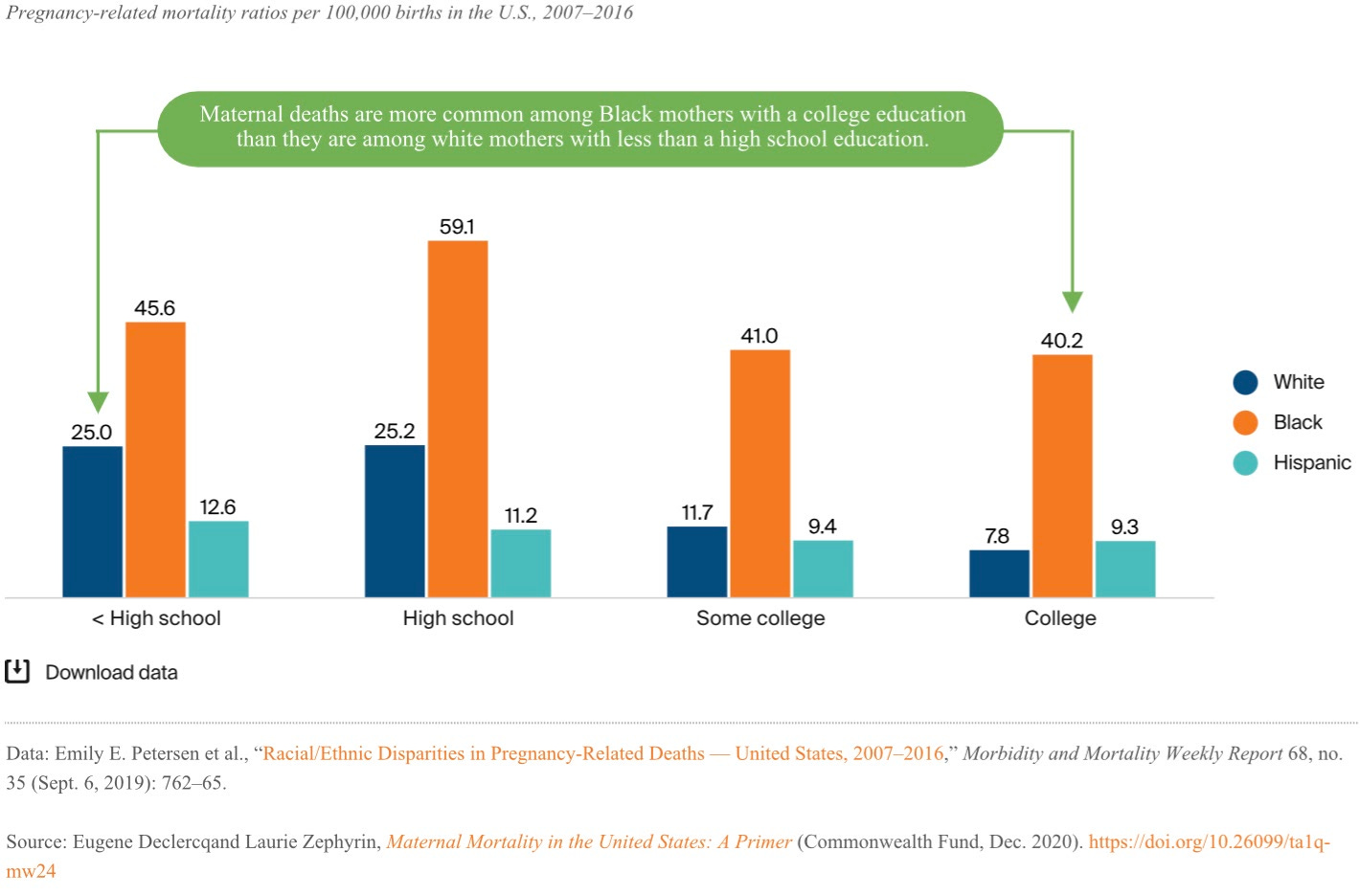
According to a Commonwealth Fund report published in December 2020, the average rate of maternal mortality in the U.S. is 17.4 per 100,000 pregnancies, the worst among industrialized countries. It’s notably worse for Black women in the U.S., who suffer a maternal mortality rate of 37.1 per 100,000 pregnancies.
The disparity is dramatic, and it persists regardless of level of education. In this chart from the Commonwealth Fund report, you can see that Black women with a college education are still dramatically more likely to die from a pregnancy-associated complication than white women with less than a high school education.
There are multiple reasons for this disparity, but there are two I want to talk about here, one that’s easier to fix with policy changes, and one which requires more of a whole system reboot.
First: Spotty insurance coverage
Although low-income pregnant women automatically qualify for Medicaid on the basis of being pregnant, it’s unclear how many women know that they have access to coverage, and how many women are actually able to access that coverage and/or find a doctor who accepts Medicaid. In 2018, almost 7% of non-Hispanic Black women didn’t access prenatal care until the third trimester. An additional 3% didn’t access prenatal care at all. Good prenatal care identifies risk factors and is as protective for the mother as it is for the fetus—so lack of it can mean doctors aren’t able to catch serious problems in time for treatment.
In many states, Medicaid for pregnant women also cuts off 60 days after the woman gives birth, dropping coverage for what is increasingly known as the “fourth trimester,” or the critical postpartum period where a woman’s body is healing from the trauma of birth.
More than half of maternal deaths occur after delivery, a phenomenon in which insurance coverage is irretrievably tied up.

The American Rescue Plan of 2021, signed by President Joe Biden into law in March 2021, provides one potential path forward. The law gives states the option to expand Medicaid coverage from 60 days to 12 months following birth, providing more postpartum women with coverage. However, because it’s an option rather than a mandate, I suspect some red states will choose not to expand coverage—which is frustrating, because Southern red states have some of the highest mortality rates.
Second: Structural medical racism
Harder to measure but no less real, a significant part of the problem is that many healthcare providers just don’t listen to Black women and otherwise treat them poorly. In one survey from 2019, nearly a quarter of Black women reported experiencing disrespect from a healthcare provider, compared to 14% of white women (with high rates also experienced by Indigenous, Hispanic, and Asian women). And the recorded instances of disrespect are...not minor, either.

Education is, once again, not exactly protective. The stories of world-class athlete Serena Williams and Shalon Irving, an epidemiologist with the CDC with two masters degrees and a PhD, show the consequences of healthcare providers just not listening. (Relatedly, a study in 2016 found that about 50% of medical students and residents hold false beliefs about Black bodies being different than white—for example, that Black people feel less pain, and that a Black person’s blood coagulates faster than a white person’s.)
There are no easy answers to this, but that doesn’t mean people shouldn’t try. One organization trying to combat medical racism is the Black Coalition for Safe Motherhood, which trains Black women how to best advocate for themselves in medical situations.
Of course, as I’m sure all would agree, an ideal solution would fix the problem rather than relying on women who are in labor to use exactly the right words to communicate.
Can we fix it?
In the last few years, a host of new companies with a focus on women’s health has appeared. These include companies like Cityblock, which treats Medicaid patients and is expanding into maternity care; Oula, which seems to target wealthier (and whiter) women, primarily in New York City, by providing them a more independent experience; Maven, which appeals to employers by providing better care that reduces costs; and the newly funded Cayaba Care, which just announced its seed round last week.
Although all of these have the potential to significantly improve the pregnancy and birth experience, Cityblock and Cayaba Care have approaches to address the two major challenges I mentioned above: spotty insurance coverage and structural medical racism.
Cityblock, which announced its intention to get into maternity care several months ago, provides high-quality treatment to a primarily Medicaid population. Because of the company’s work in navigating the confusing Medicaid system—and in conjunction with increased postpartum access to Medicaid thanks to the American Rescue Plan of 2021—there’s a real chance for Cityblock to make a difference in the lives of pregnant women on Medicaid. Depending on what the final Cityblock program looks like, it may provide support for newly pregnant women to enroll in Medicaid, OB/GYNs to provide prenatal care, and medical advocates during the birth process to help the woman feel as in control as possible.
Cayaba has a different model, one that seems more targeted at the second of the two factors I mentioned above: the structural racism of the healthcare system. For right now at least, Cayaba is solely an additional support system. The company provides social workers, lactation consultants, therapists, doctors, and nurses with the intention of bridging existing care for a majority-Black patient population. (Not for nothing, the leadership team at Cayaba is also majority-Black.) The services are mostly covered by the patient’s pre-existing insurance, and Cayaba has insurance specialists to help patients get the maximum coverage they can.

Despite their promise, these companies may struggle to get off the ground beyond their home cities, as the scaling of maternity care is constrained by the fact that a lot of it has to be delivered in person. As Chrissy Farr wrote in March, it’s hard, if not impossible, to do most maternity care via telehealth. Cityblock is based in New York, and Cayaba is starting in Philadelphia (where—as they note in their press release—Black women account for approximately 43% of all births but suffer approximately 73% of all maternal deaths). These startups may ultimately be confined to major population centers rather than providing care to more rural and suburban pregnant women.
And finally, these companies can fill a gap, but they can’t address racial justice and the societal wrongs that led to the maternal mortality disparity.
Conclusion
To have an equitable, world-class healthcare system, we have to fix these disparities. To do so will require a lot of hands-on work. Medical schools need to actively counter the false beliefs many medical students apparently hold. States need to expand Medicaid coverage past the 60-day mark and into the full year postpartum. And providers need to retrain such that they’re providing equal support and listening equally to women, regardless of race.
But until these changes are made, companies like Cayaba, Cityblock, and others are essential to at least providing support that may save women’s lives.
This information shouldn’t be taken as investment advice (obviously), and the opinions expressed are entirely my own, not representative of my employer or anyone else.