
Are infusion centers profitable? No one knows!
The billing process is way too complicated

This is a short one in deference to the holiday weekend, and because of the simplicity of the point I want to make (although I think it’s important): The infusion center status quo can’t continue.
When I said in my last newsletter that infusion center billing is complicated, I meant it. While I describe that in more detail below, the main takeaway here is that most infusion centers, particularly hospitals, simply don’t know how much money the infusion center is making or losing. The mathematics are complicated, the software is outdated, and many hospitals are apparently incapable of calculating whether infusion is a loss leader or a revenue driver.
Infusion center billing
Really only read this section if you’re a healthcare nerd like me who thinks medical billing can be interesting.
The treatments done in infusion centers span several different routes of administration, different levels of complexity, and (obviously) different drugs. All of this must be taken into account when a medical biller is working through a nurse’s notes to figure out what to bill for. Note that the following applies to billing through a patient’s medical benefit, the medical side of their insurance.
There are two parts to infusion center billing: Billing for the services, and billing for the drugs (unless, of course, the drugs are white- or brown-bagged and have therefore already been paid for—but you still have to show them on the bill, with a nominal 1 cent charge attached).
When billing for the services component, the medical biller must take into account how long the infusion took. When billing for the drugs, the medical biller must take into account much drug was used. There’s even a specific way to track the necessary drug wastage that happens when a patient needs, for example, 750mg of drug that’s only available in 100mg vials.
If a patient goes to an infusion center to get infliximab, then the drug infused through the IV, the saline used to hydrate the patient (but not the saline used to constitute the powdered infliximab), and the Benadryl the nurse pushes through the IV prophylactically all have their own codes. The saline can be claimed for reimbursement as a service, but not as a drug—unless the patient is ONLY there to be hydrated with saline. And while each of these is coded for in the same claim the provider ultimately sends to the insurer, they’re grouped under one primary code, which is intended to be the highest acuity service rendered for the highest acuity drug (the infliximab, rather than the saline or Benadryl).1
Sometimes! Depending on the patient’s insurer requirements and/or strategic decisions made by the provider, and assuming the drug wasn’t white- or brown-bagged, the drug part of the claim is processed through the pharmaceutical side of the patient’s insurance. Why are the pharmaceutical and medical sides of the insurance separate? I don’t know, why is vision insurance always separate?
My favorite part of working through the madness of infusion center billing was that after untangling ALL THAT, I came to this section on a medical billing consultant’s website:
Everything I will describe here is based on the medical benefit, fee-for-service billing methodology. In no way am I wandering into hospital outpatient (HOPD / OPPS), ambulatory surgery, home infusion, or any other class of trade.
I love how defensive this is. I feel the same way. In NO WAY do I yet understand how this process changes with an HOPD site, ASC site, or home site. In fact, I really couldn’t find resources for explaining how those sites work, which is a problem, given that my Google search autofill is populated by what seems to have been medical professionals looking for the right code to use.

Ultimately, all of this matters because sending an incorrect claim means the infusion center won’t be reimbursed, or that it will be reimbursed less than it is owed. To highlight the magnitude of how important this is for the provider’s bottom line, here’s an anecdote from a medical billing consultant that I found while researching this article:
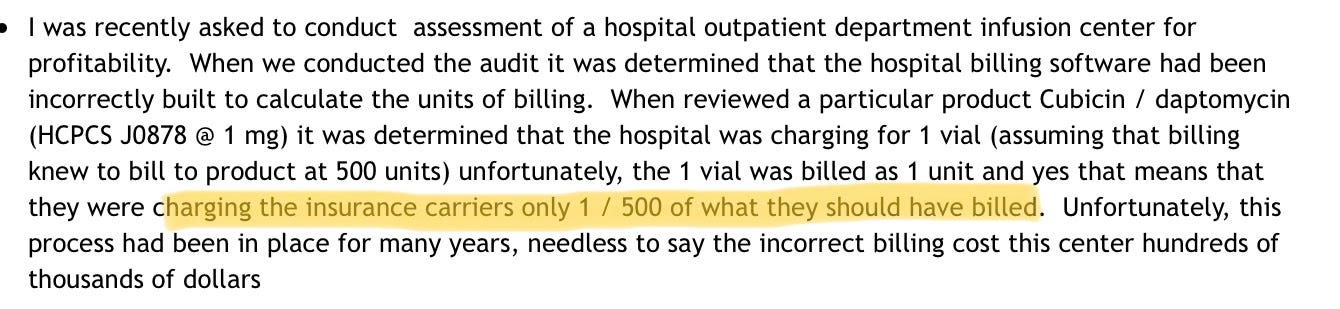
I also want to point out that the software for infusion center billing must be terrible. If the software itself was built around an incorrect unit, and the fix wasn’t clearly labeled and immediately obvious, the software is failing dramatically. I’m also going to venture to say medical billers shouldn’t have to google “CPT code for IV infusion”—that should be pretty accessible as an autofill in the software—but apparently that’s not how this works.
Which leads me into my next, less nerdy but (I think) quite important point:
The status quo simply isn’t sustainable.
Infusion centers don’t understand how much they’re making or losing
The complexity of infusion center billing and the terrible software is such that infusion centers have very little insight into whether or not they’re profitable.
It appears to be even worse for hospitals. As the Advisory Board notes, “at a typical health system, no one has full visibility into the infusion center business.” No one!
Not only does it mean that hospitals are less likely to invest in their infusion centers and/or make them more patient-friendly (because why would they! They can’t track the financial outcomes—or probably any outcomes!), it also means that the infusion business is stuck far behind other service lines, like orthopedics or neurosurgery, the kind of service lines that are so profitable that the hospital puts up highway billboards to advertise.
Instead, many hospitals seem to be floating into the new era of infusible drugs with only the barest idea of how their infusion centers are working, and with very few plans for how to make it better…mostly because of accounting issues. From a consulting website:

So yeah, if you have an infusion center and your pharmacy department appears to be unusually profitable, I guess that’s your answer?
Conclusion
As biologics continue to increase in both importance and price, and as Americans continue to live longer (once COVID starts to actually wind down), both chemotherapeutic and non-chemotherapeutic infusion will only grow in size and importance. Having a strong infrastructure in place to, I don’t know, actually track whether the hospital you run is making or losing money on a very key part of the future of healthcare seems important!
And so that’s my Labor Day rant. The whole specialty pharmacy space is behind the curve, and the billing process seems like one of the biggest obstacles to fixing that.
In other words, software might be eating the world, but a big chunk of healthcare is still on a different planet.
This information shouldn’t be taken as investment advice (obviously), and the opinions expressed are entirely my own, not representative of my employer or anyone else.
Someone knows: whether infusion centers are profitable. While I appreciate your analysis; it is unlikely that Infusion Centers would continue to be built, staffed and run if no one knew the financial bottom line.
Hi, I am currently taking a very expensive medication that I receive at an independent infusion center. The cost of the medication is extremely high and in one infusion I am getting over $60,000 worth of medication.
The reason I am writing this is that for the first 3 infusions the side effects were constant including 1 particular thing is that I would spit for at least 24 hours after receiving the drug, the other main symptom is leg cramps that are insanely painful.
I do not spit so to do so is not normal for me but every time I have received the drug I have been spitting, why I mention this, my last infusion the bag looked different meaning the amount of fluid and the color, as well as the rate of drip?
You can taste the drug in your mouth during an infusion and I couldn’t taste it at all this time, plus I didn’t feel the need to spit after the infusion and finally I haven’t had the leg cramps.
I totally am convinced that I wasn’t given the full amount of medication I was supposed to get, and seeing as it’s an 8 infusion therapy it would be extremely easy to not administer the correct dosage. Why not administer the correct dosage? Because human beings are extremely floored and it would and is all to very easy for someone to bill the insurance company for x amount of medication given and then instead of administering that amount they only gave me $10,000 worth of the drug and put the other $50,000 in their own pockets.