
The AMA is more than a trade organization
It leverages a great amount of power over key parts of the healthcare system

Last week, I wrote about how the hospital staffing crisis is becoming untenable. I argued that hospital leadership must be proactive about improving working conditions, or the crisis will only worsen.
A few readers pointed out that hospital leadership isn’t the only problem: Trade associations like the American Medical Association have become very powerful, and the AMA leverages that power in a way that can sometimes indirectly harm the very people that the AMA aims to protect.
The AMA originally formed as a professional trade society to protect the rights of doctors. Over its history, the AMA has done that. But it uses a very narrow interpretation of what those rights are; namely, it tends to prioritize physician pay over accessible patient care.
For example, the AMA has long opposed universal healthcare on the basis that it would take away doctors’ rights as artisan practitioners of medicine (and probably reimburse them less). During the Cold War, the AMA famously retained an advertising firm that created the phrase “socialized medicine” to turn public opinion against Medicare—and they used a recording of then-actor Ronald Reagan to spread the word.
Today, the AMA opposes some forms of expanded care more quietly through extensive lobbying. But the organization’s greatest power is wielded in the tight grip the AMA has over certain aspects of healthcare.
Graduate medical education
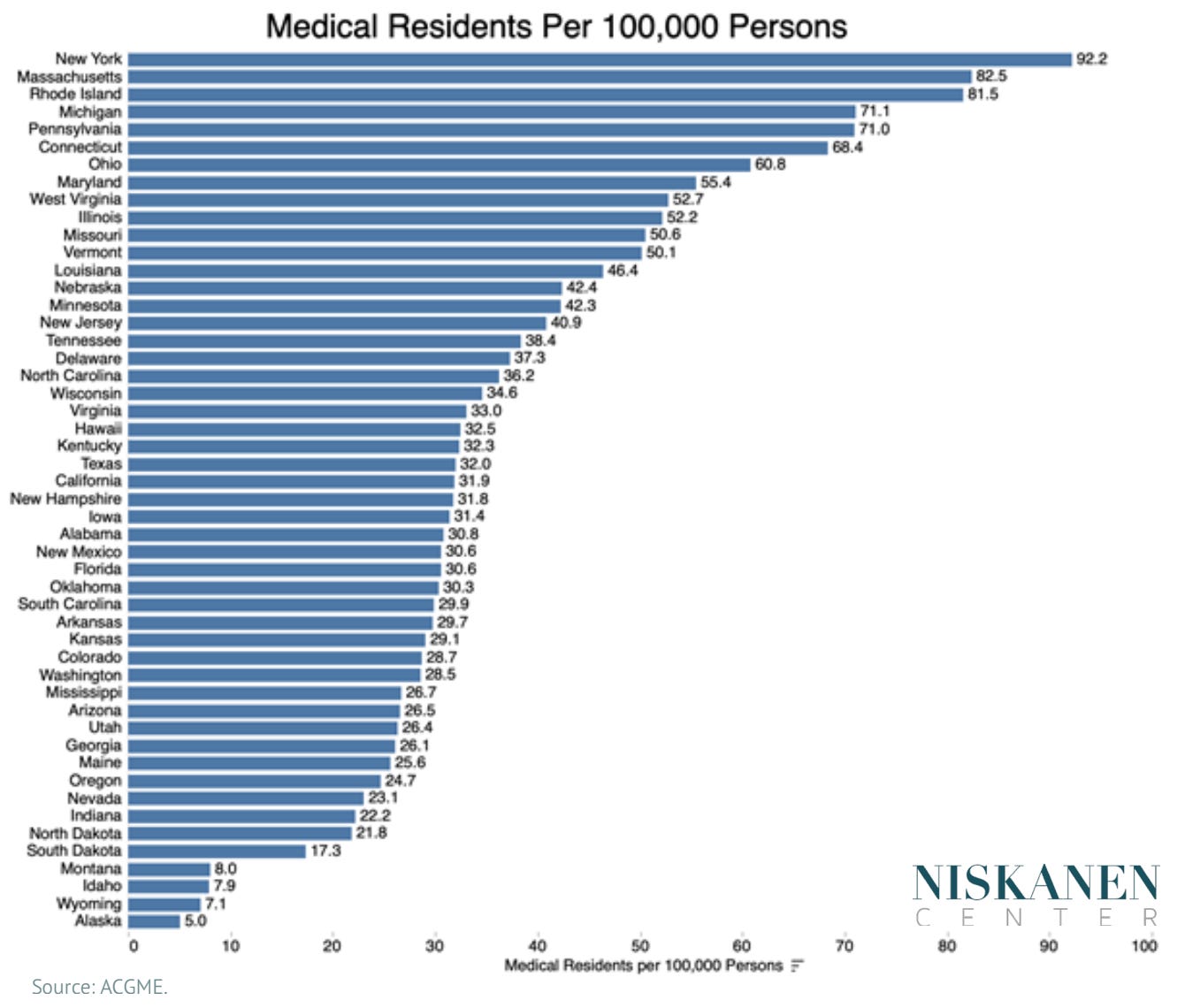
The AMA is one of the member organizations comprising the ACGME, the Accreditation Council of Graduate Medical Education. The ACGME tightly controls the number of residency slots available in the U.S., as well as controlling the process for medical students to access residency training.
The residency process was established in 1952, to put guardrails around hospitals that were increasingly pressuring medical students to sign employment contracts during medical school.
Residency funding was established in 1965; Medicare legislation allowed for payments to hospitals to help fund medical education. Some states began making payments through Medicaid as well. In 1972, the residency process became even more formalized when the member organizations of the ACGME organized to review and accredit residency programs.
Then, during the Reagan Revolution of the 1980s, several things happened to medical education. Federal support for hospital construction ended, and a federally sponsored report warned that the U.S. was facing a glut of physicians. Medical schools froze slots and the ACGME raised the standards for teaching hospitals to be accredited. In the 1990s, under Clinton, federal legislation capped Medicare’s funded residency slots at 1996 levels (and froze the slots where they were—without a provision to redistribute the slots based on geographic needs).1
In short, the ACGME, through the residency process, ultimately acted as a gatekeeper on the number of doctors the U.S. trained.
In the decades since the Reagan Revolution and the failed Clinton healthcare plan, the ACGME has been slow to respond to repeated warnings of a forthcoming physician shortage.
Some have accused the AMA and the ACGME of continuing to keep the number of slots low for anticompetitive reasons—keeping the number of slots low keeps the labor market tight and pay higher. I think it’s also likely that the AMA is too bureaucratic, and the residency process too arcane, to respond to shifts in the workforce, even when the shifts are obvious decades in advance.
The ACGME isn’t the sole entity responsible for bad working conditions at hospitals—if it was, nurses would be far better off than they are. But it’s part of the reason for short staffing, particularly in isolated geographic areas.
CPT codes
Where the AMA is more directly involved in wielding power over the healthcare industry is with CPT (Current Procedural Terminology) codes. When providers submit outpatient claims for reimbursement from a patient’s insurer, they do so with these codes. CPT codes are also the national standard for electronically transferred health data, as designated under HIPAA.
The interesting part about the otherwise dry CPT code process is that the AMA has a copyright on all of the CPT codes; only the AMA is permitted to publish the codes. Hospitals and providers everywhere have to pay a fee to have access to the CPT codes, even though these codes are essential to getting reimbursed for a large bulk of services provided.
The fee may be relatively small (I’ve seen it pegged around $17-300 per year per seat, although many physicians pay the fee bundled with their fee for EHR software so it’s not very transparent2), but the licensing fees appear to be a significant revenue source for the AMA. The AMA reportedly earns an estimated $148 million a year from royalties.
In comparison, most inpatient billing in the U.S. is coded using ICD-10 codes.3 In contrast to CPT codes, ICD-10 codes are in the public domain. The World Health Organization (WHO), which maintains the ICD-10 codes, does not charge a licensing fee.
RVS Update Committee (RUC)
The RUC is the most complicated but consequential aspect of the AMA’s power within the medical system.
Medicare reimburses CPT codes using a complex series of formulas. One aspect of those formulas is the RVS, or relative value scale. The RVS is intended to take into account the complexity, mental strain, and medical risk of each category of procedure and represent a corresponding multiple that determines how much physicians get paid for that procedure.
It actually gets even more complicated—there are three parts to every RVS, each weighted differently, and there are geographic components as well—but the important part is that it's a multiplier for a Medicare reimbursement amount. And, as with other aspects of healthcare, private insurers have copied the Centers for Medicare and Medicaid Services (CMS) and started to use some version of this system.
In short, the RVS is complicated, but it determines how much physicians get paid.
Three times a year, the physicians on the RUC meet to debate what the RVU should be for different procedures, as encapsulated in different CPT codes, which it then recommends to CMS (which typically, although not always, accepts the recommendations). The AMA originally formed the RUC and manages the process.
The RUC can be dicey in a few different ways. First, it’s comprised of doctors. The prices that doctors get paid are...set by other doctors. (It’s a further illustration that healthcare isn’t exactly a normal marketplace, given that consumers have to pay the price that a small subset of doctors set, in some way, for all the doctors across the country.)
Second, primary care doctors have alleged that the panel tends to have a disproportionate number of specialists. A RUC stacked with specialists essentially guarantees that procedures get reimbursed more favorably than office visits. This has negative consequences for the long-term, grinding work of maintaining public health, a process that ideally includes smoking cessation counseling, dietary assistance, and other time-intensive but non-procedural services that are poorly reimbursed thanks to the RVS determinations recommended by the RUC.
Conclusion
As I discussed with Stacey Richter of Relentless Health Value during my recent podcast episode, healthcare is fascinating and frustrating because there are few clear “bad guys.” Instead, the system is an amalgam of complicated incentives.
The clearest way to evaluate a stakeholder is by looking at the situation from a patient perspective: What does this mean for the patient?
In the AMA’s case, it’s a mixed bag. On one hand, the AMA has helped standardize medical training for more than 100 years. On the other, the AMA partially controls residency slots, makes hundreds of millions of dollars a year on licensing fees for an essential billing mechanism, and has perpetuated the primacy of specialists over generalists. All of these have served to harm independent physicians, keep the physician labor market tight, and otherwise make it more difficult or complicated for patients to receive care. Reforming these aspects of healthcare requires getting the AMA on board.
This information shouldn’t be taken as investment advice (obviously), and the opinions expressed are entirely my own, not representative of my employer or anyone else.
If you want greater detail, the Niskanen Institute, a moderate, libertarian-flavored think tank, recently put out a good history of how we formed residency slots.
One caveat is that, while their history is good, you can sense the libertarian flavor in their repeated mention of physicians being motivated by salary. Maybe it’s true in part, but frankly, if physicians were primarily motivated by money, I suspect they’d go into finance.
Optum360 is apparently the vendor that collects licensing fees for CPT codes on behalf of the AMA, just an interesting tidbit.
Medicare reimburses ICD codes using a process that rolls ICD codes into DRGs, or diagnosis-related groups, and then reimburses based on a complex formula—which is a whole separate process that’s worth reading about but is beyond the scope of this piece.