
What will doctors do now?
30% of healthcare workers want to leave medicine. Now what?

TW: healthcare worker mental health challenges and suicide.
I started this newsletter about 9 months ago (!) with a piece called “What will doctors do now?”
I conceived of the piece as asking what physicians would do after COVID, given the additional frustrations and strain that COVID seemed to put on physician/hospital relationships. The topic seemed particularly pressing because, as I briefly mentioned last week, physicians’ relationships to the health systems where they work has been an interest of mine—and because those relationships seemed increasingly contentious even before COVID.
But when I talked to two doctors, Dr. Andrew Goldstein of the group Progressive Doctors, and Dr. Eric Topol, who helped launch the group Medicine Forward, they both seemed a bit more hopeful about the future than I expected.
Dr. Topol spoke of increased physician solidarity:
It isn’t just one issue. There was the [physician] burnout, there is the pandemic, there is the other virus of racial discrimination, and all of this together is, I think, bringing the physician group, hopefully, to rise and come together to confront it meaningfully, in solidarity.
And Dr. Goldstein talked about the dichotomy between the depths of the pandemic and the apex of feeling inspired by the many health workers who assisted in the protests following George Floyd’s murder last summer:
I’m neither hopeful nor pessimistic based on what I saw transpire, because it was both so much better than what it could’ve been, but so much worse than it could’ve been.
When I finished writing that first newsletter post, I came away with the sense that the crucible of the pandemic might force hospitals to treat healthcare workers with more respect and autonomy, and that healthcare workers might find a new voice in advocating for preparedness, adequate supplies and staff, and racial equity in care.
The pandemic and healthcare workers
This is particularly poignant and necessary given a recent survey from the Washington Post and the Kaiser Family Foundation about how much the pandemic seems to have burned out and depressed American healthcare workers.
More than 60% of surveyed healthcare workers reported that the pandemic had had a negative effect on their mental health, and almost 50% reported a negative effect on their physical health.
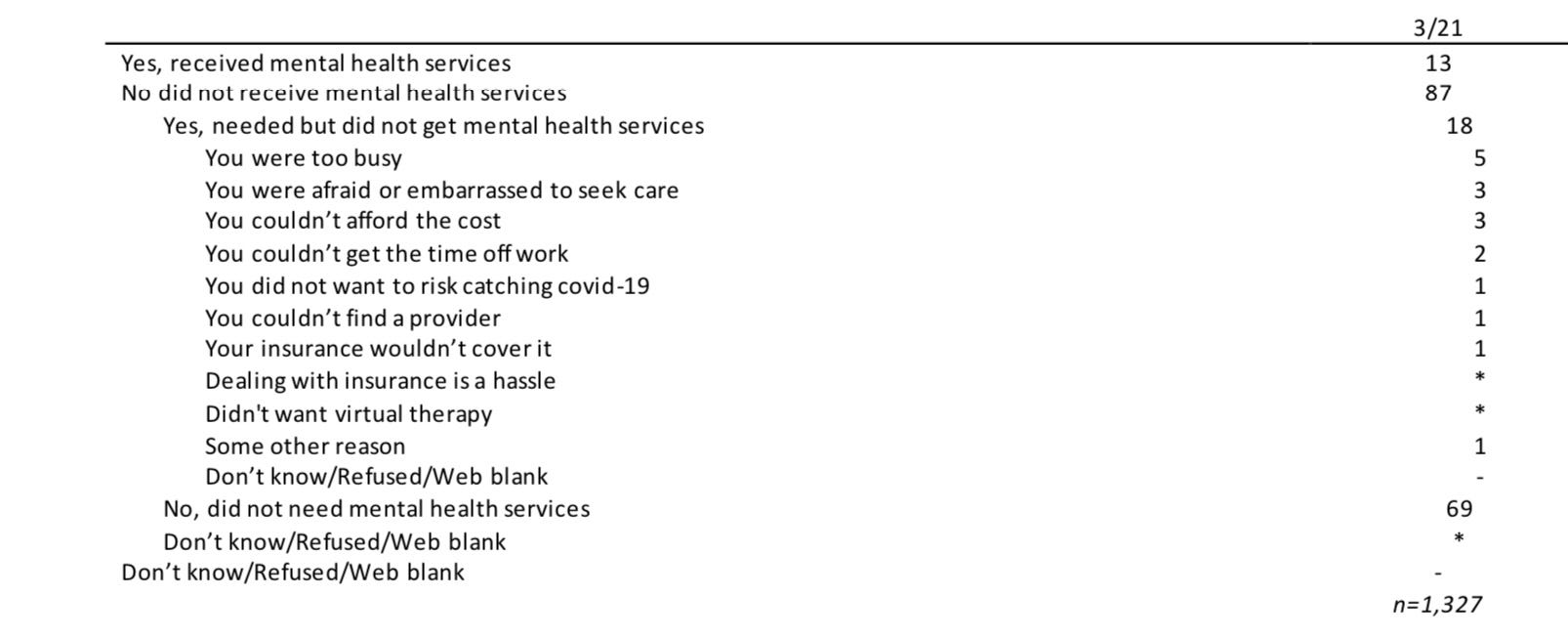
The survey also asked for details on whether these workers sought healthcare, and if they did not even though they felt they needed it, what had stopped them. Of the approximately 30% of healthcare workers who said they needed mental health care, only around 13% of them actually got care. I included the full crosstab table below.
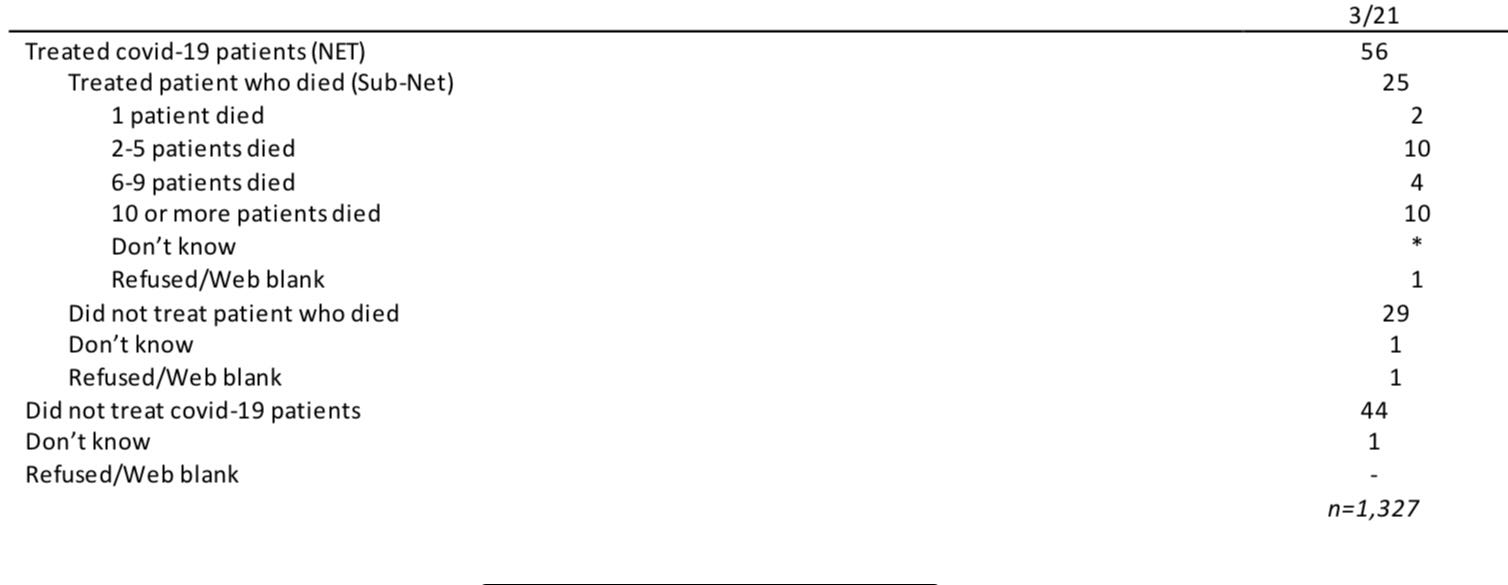
The survey also asked healthcare workers whether they treated COVID patients and, if so, how many of the patients died.
Less scientifically but no less poignantly, this Reddit thread has thousands of responses from self-identified healthcare workers who are burned out.
And perhaps unsurprising, after all those statistics, but very important: 30% of healthcare workers surveyed by WaPo and KFF want to leave medicine altogether (the Washington Post wrote this statistic from the survey up into a fuller story, which is worth reading). That’s a huge number!
Having this many healthcare workers who want to leave medicine is unsustainable. The Association of American Medical Colleges projects a shortage of up to 139,000 physicians by 2033. The Bureau of Labor Statistics estimates that there will be 175,900 openings for RNs every year through 2029, counting increased need, alongside retirements and workforce exits. Losing 30% of the existing workforce years before their expected retirement date would certainly exacerbate these shortages.
Finally, I can’t write this without acknowledging the suicides of healthcare workers directly linked to the pandemic. There have been a few, heartbreaking profiles of healthcare workers who were simply overwhelmed by the superhuman task—saving lives in a novel pandemic without enough supplies, staff, or space.1 And undoubtedly there are even more whose struggles were not covered.
What will doctors do now?
So here we are. As the baby boomer generation retires, there will be a need for healthcare workers to both treat the aging population and backfill for when baby boomer healthcare workers themselves start to retire. But there’s already a shortage of medical residency slots. Becoming a healthcare worker requires a long period of expensive schooling before most providers can be licensed, which makes the process more challenging for people from lower-income backgrounds. The healthcare workers we need most—nurses, primary care providers, etc.—are underpaid relative to more specialized professions. And, of course, the aforementioned effects of the pandemic will likely play a role.
Fixing these problems requires national policy changes, which means it’ll probably continue to be a problem until a legislator notices that it’s hard to get a doctor in a few years. But in the short term, I think a few things will happen:
Already-independent physicians will try to stay independent. This is contrary to one of my earlier predictions; I expected independent providers to be weakened by the pandemic’s cut on elective visits and procedures, and I expected these practices to be strongly compelled to merge with health systems. But it looks like that’s not happening—and I suspect it’s because the remaining independent providers really value their autonomy.
Relatedly, more physicians and physician groups will seek new partnership opportunities with health systems that stop short of full acquisition. On a recent Radio Advisory episode (which is relevant and worth listening to in its entirety), the hosts noted that they’re seeing more inbound from both health systems and provider groups who are looking for innovative ways to partner, while maintaining autonomy.
More healthcare workers, especially those not affiliated with existing practices, will find 1099 contracting appealing. As I’ve mentioned briefly in the past, at least a few existing mental health startups use therapists who are 1099 contractors, meaning they are not full employees and can take on a varying number of client hours a week. Healthcare workers burned out by the constant stress of the pandemic, and unable to return to crowded city emergency rooms, might find a way to keep practicing medicine on their terms in the 1099 relationship.
What will hospitals do now?
Health systems hold a unique fascination for me, partially because I started my career at Advisory Board, and partially because I wanted to be a doctor for so long (I was job shadowing in hospitals when I was 13). But mostly it’s because hospitals are a holdover of an earlier age, an age of primarily acute illnesses and injuries, and yet hospitals remain the primary setting in our current system to receive emergency or longer-term, high acuity treatment.
And I’ve gone back and forth on whether the future is a future without health systems, in their current form, at all. When a16z put out their post declaring that “healthcare has left the building,” during the pandemic, I didn’t know what to make of it. Wasn’t the pandemic the foremost example of how we need excess reserve hospital capacity at all times, for just such crises?
But at the same time, hospitals are something of an anachronism. If healthcare workers don’t enjoy working there, it wouldn’t take that much more to, I suppose, unbundle all or most of the important aspects of a hospital into different companies or clinics. For that matter, should immunocompromised cancer patients share a hospital with new babies, trauma victims, people with influenza, and those recovering from surgery? And, if we’ve learned anything from COVID, isn’t it that infectious disease should be housed away from the very young and the very old, the immunocompromised, and those who have afflictions that aren’t infectious?
I don’t have an answer, but regardless of the outcome, I can’t help but think that the landscape is inevitably rolling towards change. COVID accelerated a lot of things, including the breaking of the existing healthcare system; it was bad before COVID, but—if the above healthcare worker survey is any indication—the damage is accelerated now.
As always, let me know your thoughts by commenting below or replying to this email. And if you agree, disagree, or have further thoughts—I’d love to hear it.
This information shouldn’t be taken as investment advice (obviously), and the opinions expressed are entirely my own musings, not representative of my employer or anyone else.
*Staff, stuff, space framework is from Dr. Paul Farmer’s book Fevers, Feuds, and Diamonds: Ebola and the Ravages of History.